
First, a small rant. Anatomy in Motion is NOT just about the feet.
An assumption often made about the world of Anatomy in Motion is that everything we do is about working with the feet. The feet are the root of all problems and all we do is get people to pronate and magically they become pain-free.
Wrong. Not problem is a foot problem.
Well, not 100% wrong. Every problem is in some way related to the feet, but only because every body part is related to every other body part.
A problem with anything can become a problem with anything else. If you change one thing in the body, everything else must change in response.
AiM is not all about the feet. More accurately would be to say that AiM is all about understanding how everything affects everything, and the role of the feet is often so neglected and underappreciated. AiM gives us by far one of the most comprehensive biomechanical models of foot pronation and supination, and how these specifically coordinate with every other joint in the body, allowing us as practitioners to make meaningful connections between the feet and the rest of the body.
But not every person’s problem will need to start by working with their feet.
And my case study today is a great example of this.
Watch the video and read this case study and you’ll get to see how working with a chest scar and exploring shoulder and neck movements created a change that was observable all the way down to the feet.
It was pretty cool, and I hope you’ll think it’s cool, too.
Ready? On to today’s case study…
Meet Jon
Jon has generously donated his body for your learning pleasure. Thanks, Jon!
I first met Jon in 2023 when he took the AiM Closed Chain Biomechanics course I taught in Toronto. He is a keen learner of AiM and I always love a good movement nerd-out with fellow students.
Jon’s main goal in our session (other than wanting to expand his awareness of his own movement patterns and learning the Flow Motion Model), was to understand the source of his right side lower back discomfort.
He also noticed it was more difficult to get his weight to go into his left leg while walking.
Keep those in mind as we journey forward.
Assessment
A big stand out for Jon came to light in our chat about his past medical history.
He rattled off a list of things… An old ankle sprain whilst trail running. A back injury that started after a lift in the gym gone wrong.
But what stood out in a big way was that he had a scar on his right side of his chest, right under his clavicle.
He shared that when he was a kid he was in the hospital for leukemia treatment, and that scar was from where he the port put in.
He told me that last January while at an AiM course with Gary Ward in London, they had briefly assessed his scar’s impact on his whole body movements, but they didn’t really have the opportunity to get into it deeply enough to come to any conclusions.
Spoiler alert- His scar was affecting his movement in a big way.
And we’ll get into the details of that. But first…
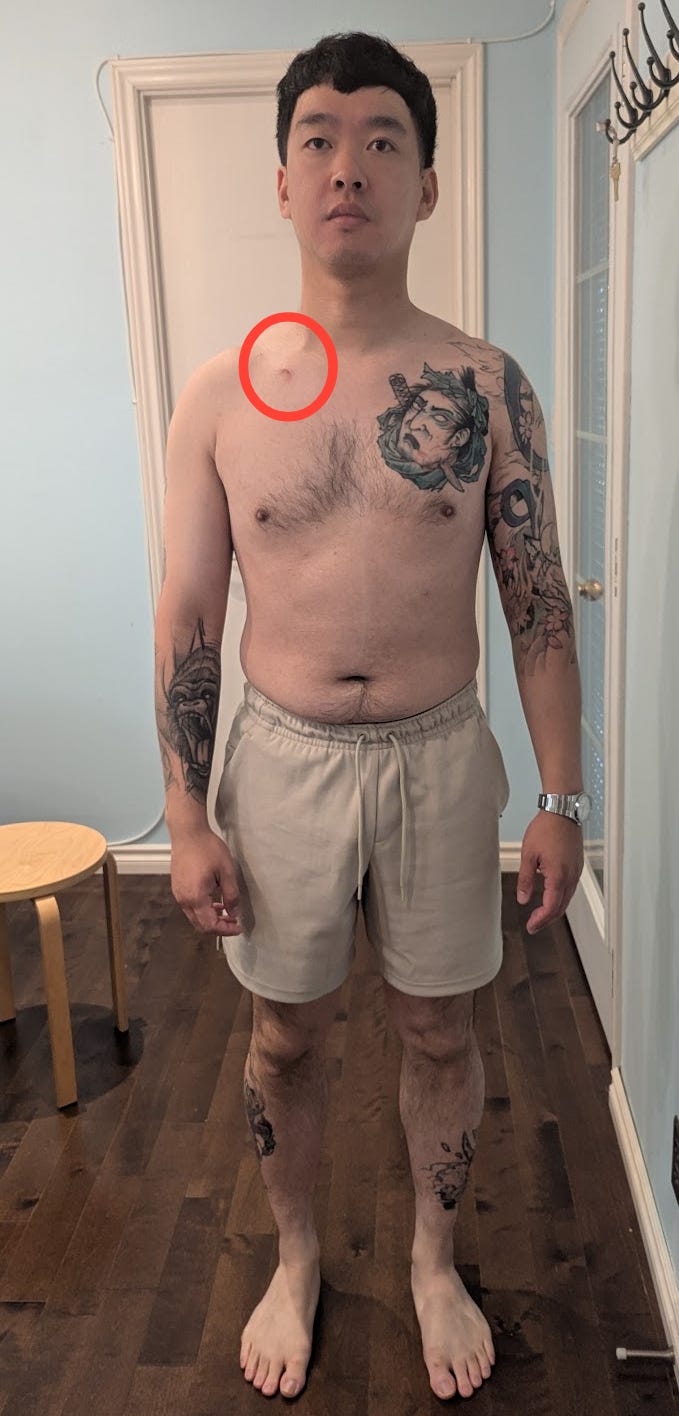
Here’s a picture of his static alignment from our initial assessment:
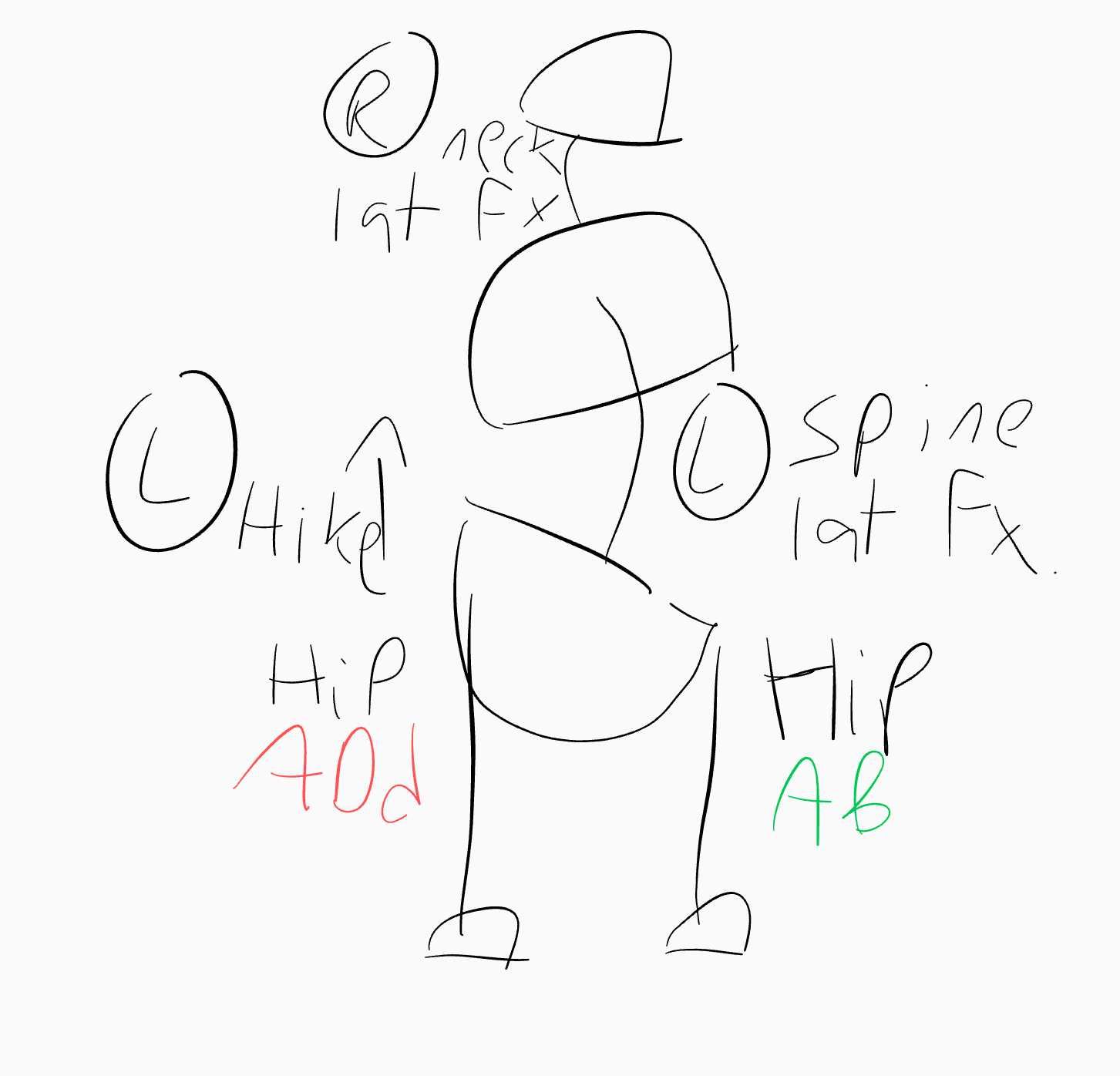
Notice his pelvis hiked on the right, with a right lateral flexion and rotation in his spine. This is likely to be the correlation with his lower back pain on the right. The space there being more closed and compressed.
We can also understand how this alignment will generate a hip adduction on the right, and abduction on the left, which is correlated with his felt sense of not being able to get his weight as easily onto his left leg.
What I also think is quite interesting is how his posture is organized around closing in around the area of his clavicle scar:
Spine lateral flexion to the right
Spine rotation to the right
Right shoulder more internally rotated
Those mechanics will effectively close down movement through his scar area.
Gait and dynamic assessment
What was interesting to see in his gait was that he also struggled to access the movements that his body wasn’t accessing in his static alignment:
Pelvis hike left and thus left hip adduction
Spine lateral flexion left
Neck lateral flexion right: His neck stayed in his left lateral flexion throughout every phase of gait.
His neck in particular became a curiosity to me.
In the Flow Motion Model, in order to full weight-bear into your left leg we need the neck to laterally flex to the right.
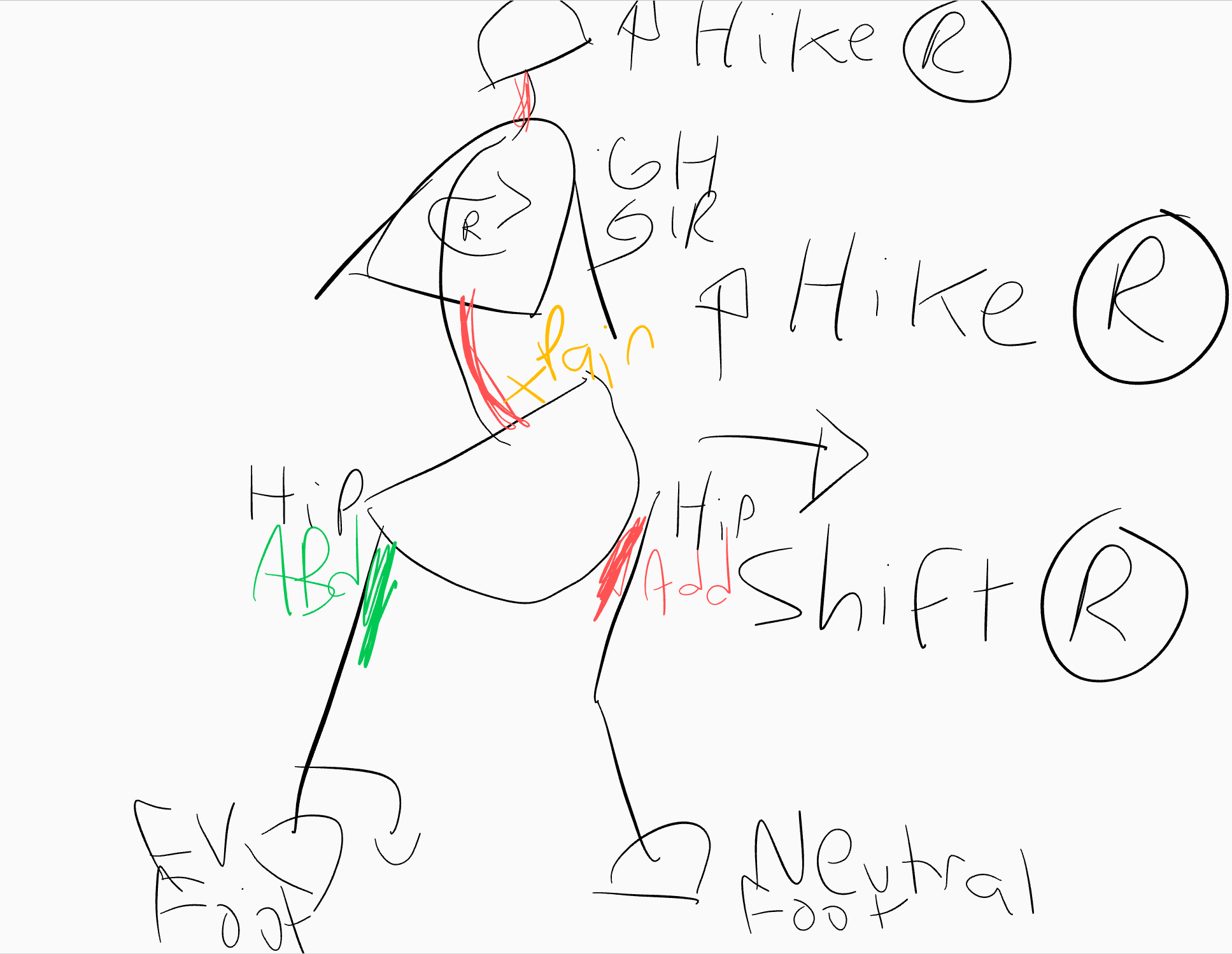
Jon was missing the whole body shape we see at this moment in time, which looks like this:
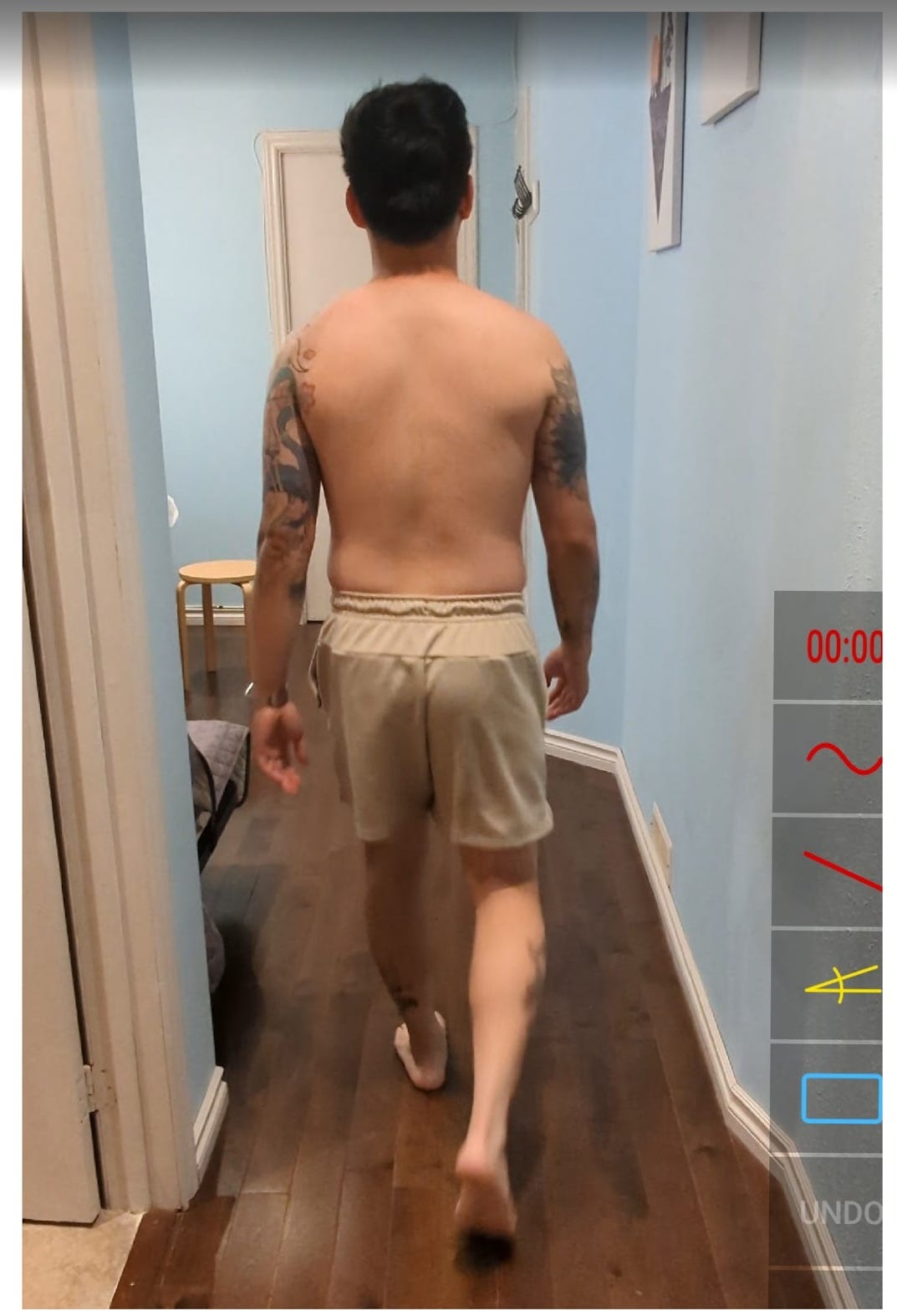
And check out the screenshots below of his suspension phases from his before gait video, and notice how his head is ALWAYS in a lateral flexion to the left (right ear higher):

Check yo neck (and yo chest scar)
Remember that chest scar?
One thing we know about scar tissue is that it lays down thick and strong to limit movement so the area can heal.
And if our bodies are neve taught to move through an area with scar tissue, ideally as soon as possible after wound healing, then the likelihood of it happening on its own is pretty low. Its a very useful protective mechanism our bodies have.
Its almost as if, to our unconscious bodies, the scar becomes a no-go zone for movement. All movement happens around the scar, not through the scar.
It would make good sense for Jon’s body to take on his current body position so that the wound in his chest could heal without getting constantly pulled open again, all those years ago.
But now, present day, wound healed, how well are the structures around his thoracic spine, neck, and shoulder able move? Are they in this disorganized position as a result of adapting to the healing of his chest wound? Are the adaptations his body made around his healing scar decades ago still keeping him stuck with his current pattern and problems?
And will encouraging better quality movement there help things below in his back, hips, and feet?
Testing the hypothesis, testing the scar
In our dynamic assessment the main stand out “missing movements” we discovered were:
Right scapula protraction (maybe it is already stuck protracted?)
Left pelvis hike with weight getting onto left leg, i.e. left hip adduction (because his pelvis is already in a right hike and can’t get to the other side?)
Skull lateral flexion right
The difference in his scapula protraction was so noticeable that we made a video (check the after video at the end of this post!):
To test if his scar was interfering with these movements we played a little scar stretch game.
With any scar, you can test and see if it feels limited when stretched in a particular direction. Drag the tissue up, down, left, right, and on diagonals, and you’ll find a vector of pull that feels stickier.
For Jon, his vector of barrier, the most sticky direction to stretch his scar, was directly medially towards his midline.
As a test, I dragged his scar towards his midline, then got him to recheck his pelvis hikes, neck lateral flexion, and scapula protraction, and, lo and behold, BOTH improved.
It was a little freaky, but the information this gave us was that YES, his scar and ensuing healing process around it is linked to his current jumble of missing and disorganized mechanics.
Our goal? Give them back in an organized way and treat his scar so movement can pass through that area again.
How? Mobilize that scar and give the missing movements back with some thoughtful and specific exercises.
What we did
We did two exercises.
Arm spirals. The intention was to explore his right scapula protraction with shoulder internal rotation, and let that feed movement into his spine and neck. While he performed this movement, he also stretched his chest scar towards his mid-line with his left hand.
See how you do with this arm spirals exercise (clip from my Liberated Body workshop):If you followed along with that movement in your own body, you’ll have felt how your right arm internally rotating generates both a spine rotation and lateral flexion to the left. And by keeping your eyes on the horizon and head level, your neck would experience an oppositional lateral flexion to the right. These were the missing motions we wanted to give back to Jon.
After the arm spirals, we re-filmed Jon walking, and noticed a some subtle changes.
Check out the snapshot below:

Jon subjectively reported feeling slightly better access onto his left leg, which is great, but I knew we needed to get his head integrated with his body below as it STILL was stuck in that left lateral flexion.
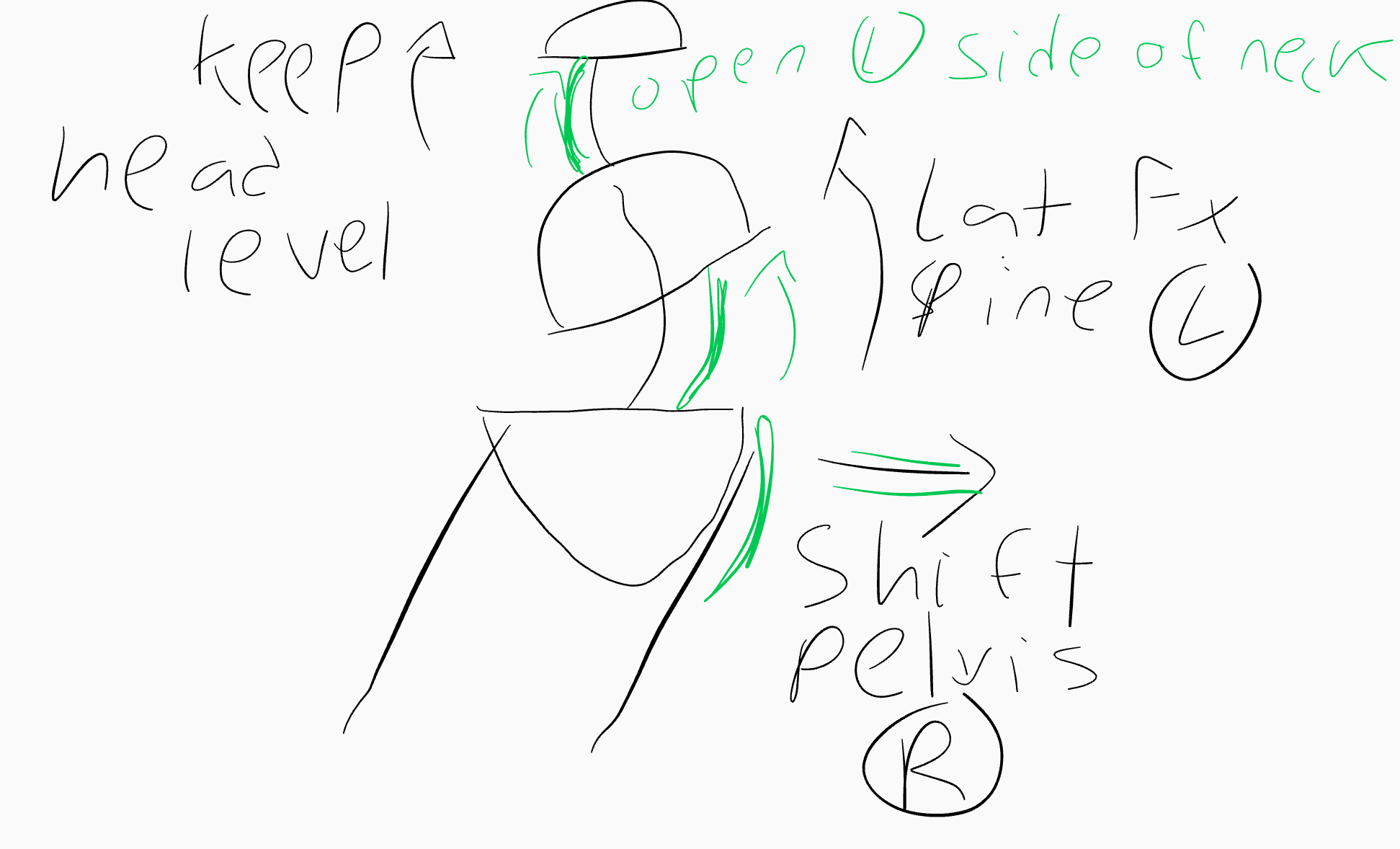
So we decided to explore a second movement to focus more directly on opening up the left side of his neck and give back the missing right lateral flexion.
Off axis pelvis shift right with neck lateral flexion right. The intention was to explore his access to neck lateral flexion to the right via the pelvis shifting and generating a spine lateral flexion to the left.
We did a movement that looked like this: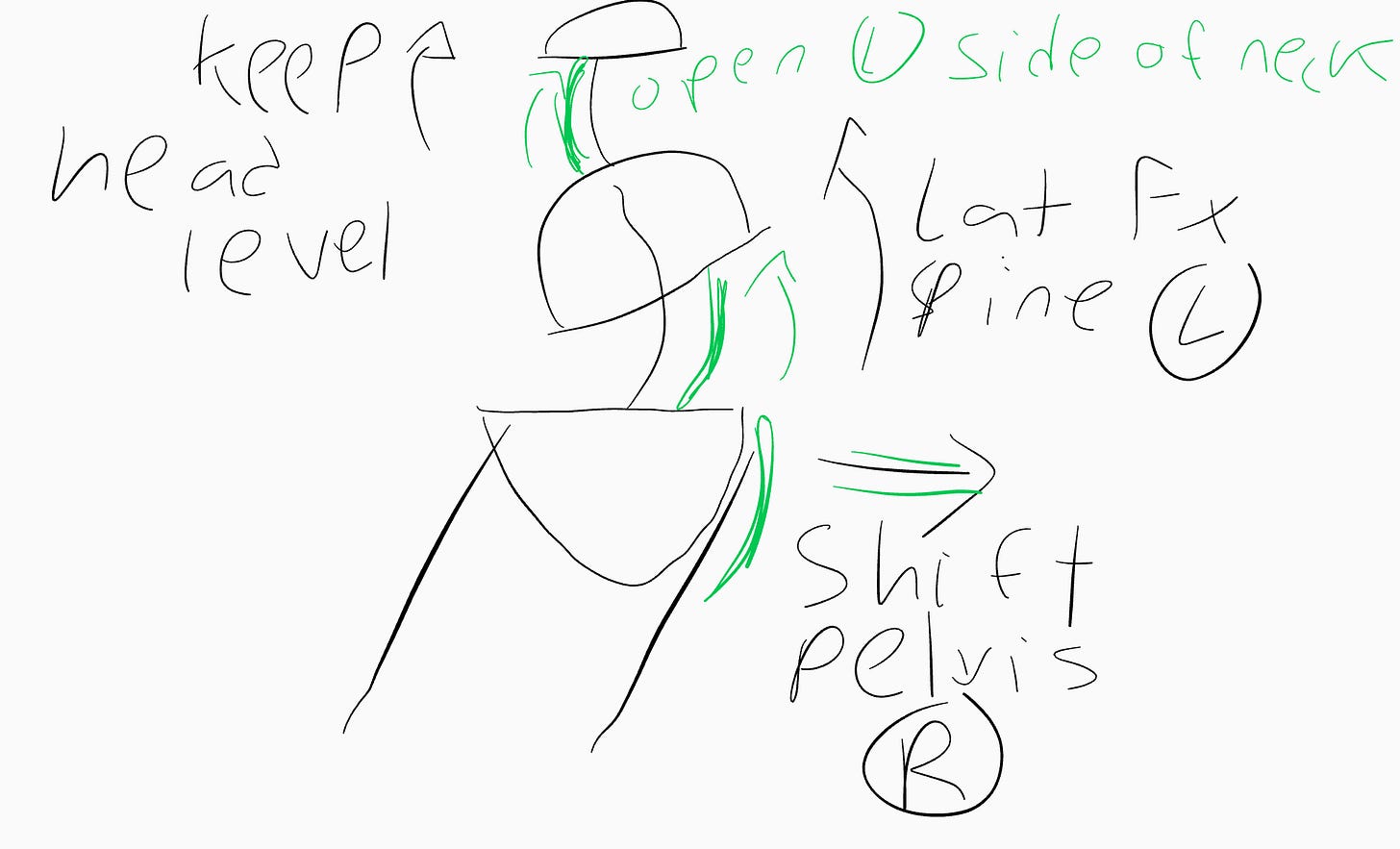
Why didn’t we just do a plain old ear-to-shoulder static neck stretch? Why make it a whole body movement? Glad you asked.
We explored his neck in this way is because of how in our walking cycle, the way our neck experiences lateral flexion is by staying still, eyes on the horizon, and our spine moves underneath it.
Here’s a little visual of that as a concept (clip from an online movement lesson on neck mechanics):This oppositional motion between the neck and spine is KEY for having symmetrical access to both side of your body as you walk.
If Jon can’t laterally flex his neck to the right, then he won’t have great access to many of his missing mechanics, such as:Pelvis hike left
Spine lateral flexion left
Left hip adduction
Stepping his left leg forward
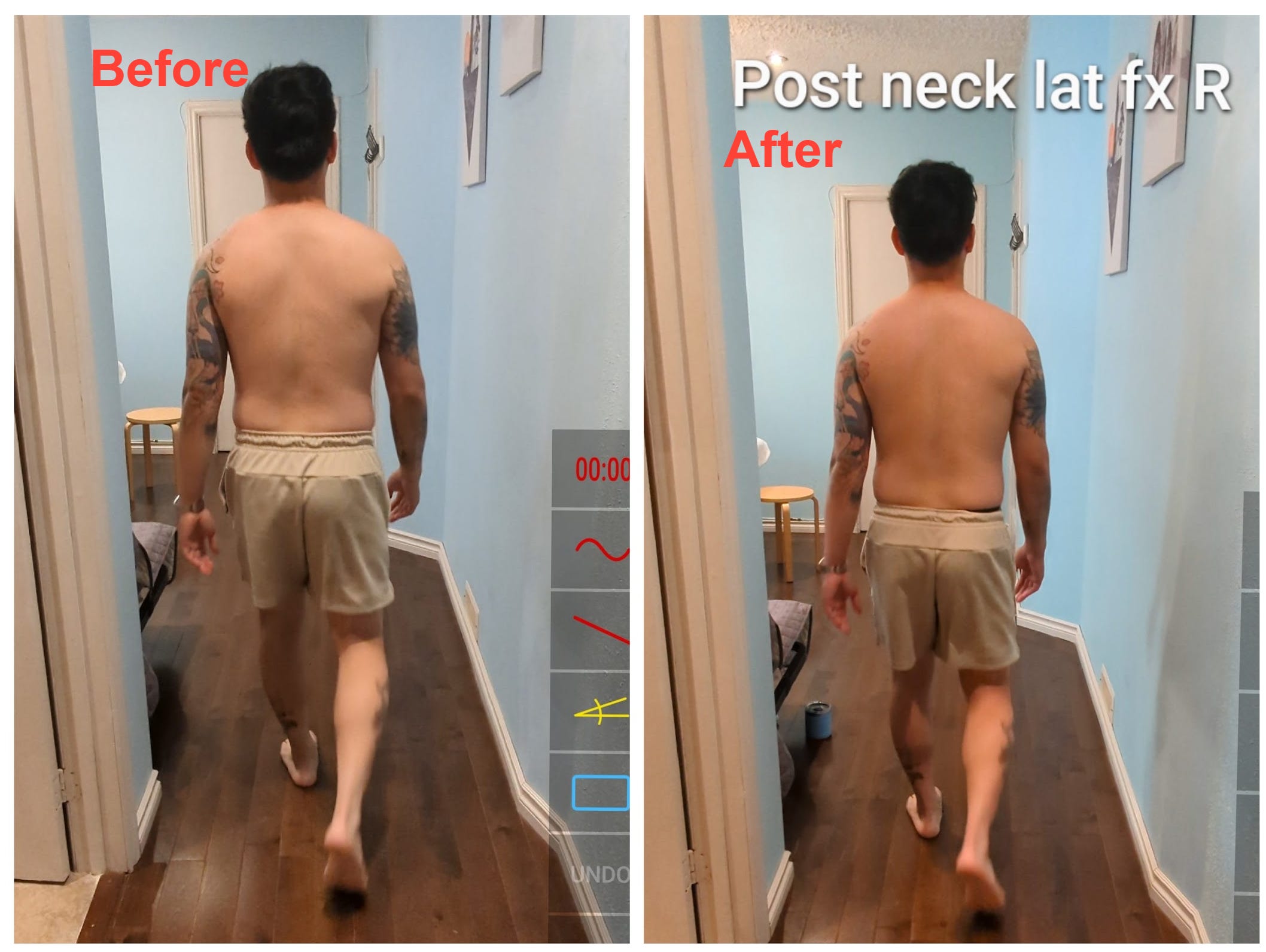
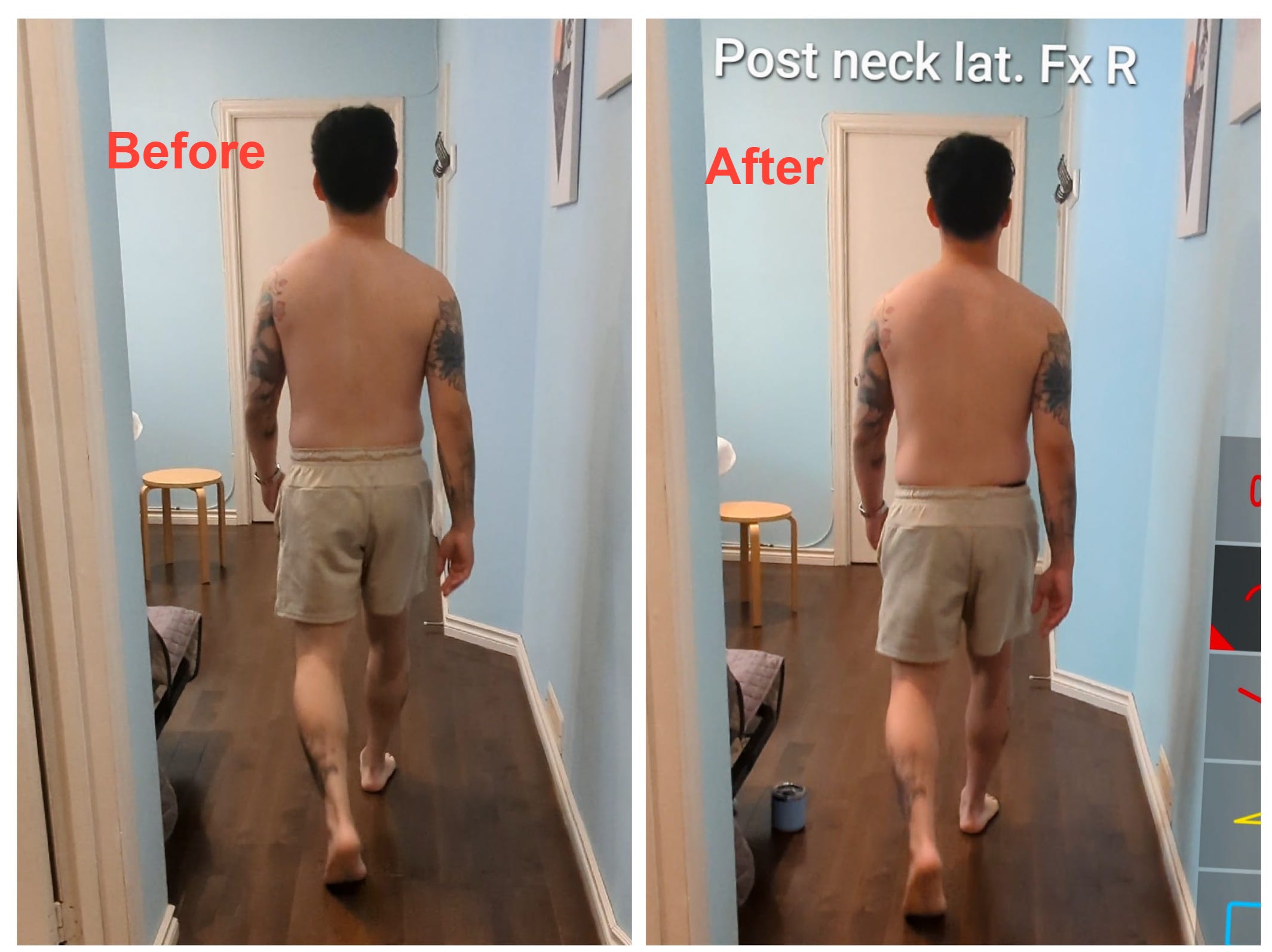
Exploring neck lateral flexion right gave us some more cool changes. Check out these snapshots from his walking after working on his neck lateral flexion to the right:
Re-assessment
Jon reported feeling more centered with his head position and an even better sense of getting weight through his left leg. Win!
He also had better access into his left hike. In theory, this will correlate with an improvement in his right sided lower back pain, as he is able to move out of that compressive right pelvis hike he was originally stuck in, and access the opposite shape to the left, opening the compressed area.
Ready for his scapular protraction after video?
Pretty cool to see that evening out, which will also help him access more symmetrical spine and shoulder movements through his gait cycle.
I also love seeing a subtle change in his feet. That said, his left foot still stands out to me as an area that will need help as his next step in the process, having had a pretty gnarly sprain. Hopefully Jon will be able to give us some updates on his progress going forward!
Final thoughts?
A few key take-aways to reiterate:
It’s not always about starting with the feet. In Jon’s case, we started at his neck and right shoulder to get a change in his body below. The important thing is to understand how the feet connect with the rest of the body, affecting it and affected by it. But we don’t have a rule in AiM of needing to help the feet first.
Scars can have such a profound impact on our ability to access our mechanics around that area. Always check the impact of a scar. Often the body will reduce movement through that area. Not all scars mess with our movement, but it is always good to check.
When you see a part of the body that stays in the exact same position throughout every single phase of gait (Jon’s neck), it is likely to be a good place to begin restoring missing movement potential. Especially if that is an area where there’s been an old injury that’s been untreated and unconsidered. In Jon’s case, a port put in.
I hope you enjoyed this case study! Stay tuned for more like this. I’ve been by at at least 3 people that they find these write-ups useful, so I’ll keep going, just for you.







